More Than a Sleep Hormone
Melatonin is a crazy powerful hormone and molecule. It is often relegated to sleep enhancement and is left there, which means most people are sitting on something genuinely remarkable without knowing it. The antioxidant properties alone would warrant a lengthy article. Not to mention the anti-inflammatory signaling, the mitochondrial protection, the emerging longevity data. Sleep is the least interesting thing it does.
One of the most underrated effects is what melatonin does to growth hormone output, particularly at higher doses and particularly when you’re already running a growth hormone secretagogue. The mechanism is specific, the human data go back to 1970, and a 2025 case report shows the effect holding up chronically in a real-world setting.
Dosing is all over the place with melatonin, but that conversation usually stays anchored to sleep. This article isn’t about sleep. It’s about growth hormone, how melatonin amplifies it, why the mechanism makes sense, and what it looked like in my own labs when I ran the stack.
The Longevity Case for Melatonin
Your body makes melatonin in the pineal gland, a structure about the size of a grain of rice sitting near the center of your brain, and it starts releasing it when light drops off at night. Most people know that part. What gets less attention is what melatonin is doing at the cellular level, in places that have nothing to do with whether you fall asleep faster.
Melatonin is one of the most potent antioxidants your body produces. It concentrates directly inside mitochondria, the structures inside your cells that generate energy, and it neutralizes free radicals there before they can damage the machinery keeping those cells functional. Most antioxidants you take orally never reach mitochondria in any meaningful concentration. Melatonin does, and the evidence for this is well established.
Melatonin suppresses NF-kB, a signaling molecule that acts as one of the primary switches for chronic inflammation, across multiple tissue types. Chronic low-grade inflammation is one of the better-characterized drivers of accelerated aging, and melatonin is interfering with it at a mechanistic level.
There is also a growing body of animal and early human data suggesting melatonin helps preserve mitochondrial function as we age, which translates directly to how well your cells produce energy, recover from stress, and maintain tissue integrity over time. That’s the longevity angle, and it’s a standalone argument for melatonin before you ever get to growth hormone.
What Melatonin Does to Growth Hormone on Its Own
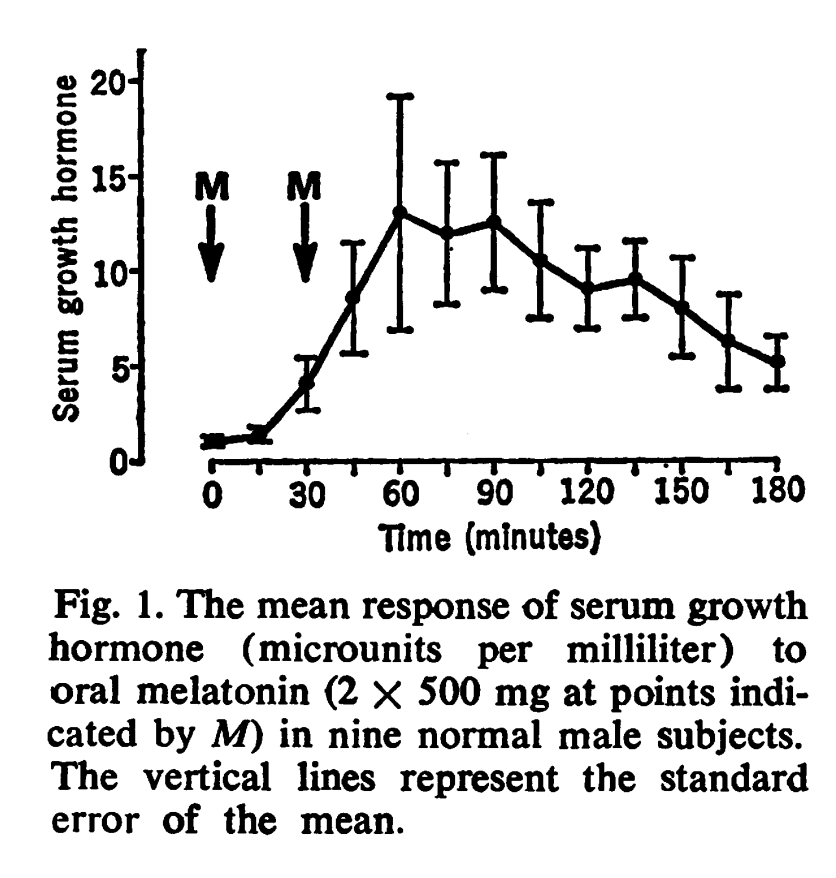
In a 1974 study, researchers gave nine healthy men a single gram of oral melatonin and measured what happened to their growth hormone over the next several hours. Eight out of nine showed a significant GH rise, with peak levels reaching into the 20 to 25 μU/mL range. That’s not a modest nudge. That’s a response you’d expect from a pharmacological stimulus, produced by a molecule most people associate with jet lag.
The effect isn’t limited to gram-level dosing. Studies using 0.5 mg and 5 mg show melatonin modulating nocturnal GH patterns at doses well within the range of what people are already taking. The signal is weaker at those doses, but it’s there, and it’s consistent with melatonin playing a real role in how your body regulates GH during sleep rather than just coincidentally being present at the same time.
The most striking data point in the recent literature comes from a 2025 case report published in JCEM Case Reports. A young woman taking chronic over-the-counter melatonin developed persistently elevated GH and IGF-1, the downstream marker that tells you GH has actually been doing its job in the liver and peripheral tissues. She had no clinical signs of acromegaly, and her levels normalized within about a month of stopping melatonin. What that case shows is that the GH effect of melatonin isn’t just an acute laboratory phenomenon. It can sustain chronically at real-world doses, and the axis doesn’t appear to be adapting away from it during use.
The Somatostatin Mechanism: Releasing the Brake
To understand why melatonin amplifies GH output when you’re running a secretagogue, you need a basic picture of how GH secretion is controlled. Your pituitary gland releases GH in pulses, and two hypothalamic signals compete to determine how large those pulses are. Growth hormone releasing hormone, or GHRH, is the signal that tells the pituitary to fire. Somatostatin is the signal that tells it to hold back. The size of each GH pulse is largely determined by how much somatostatin is present at the moment GHRH arrives. High somatostatin tone means a blunted pulse, and low somatostatin tone means the pituitary responds fully to whatever GHRH signal is coming in.
Melatonin reduces hypothalamic somatostatin tone, which means more of the GHRH signal gets through to the pituitary and produces a larger GH pulse. You’re releasing the brake rather than pressing harder on the accelerator.
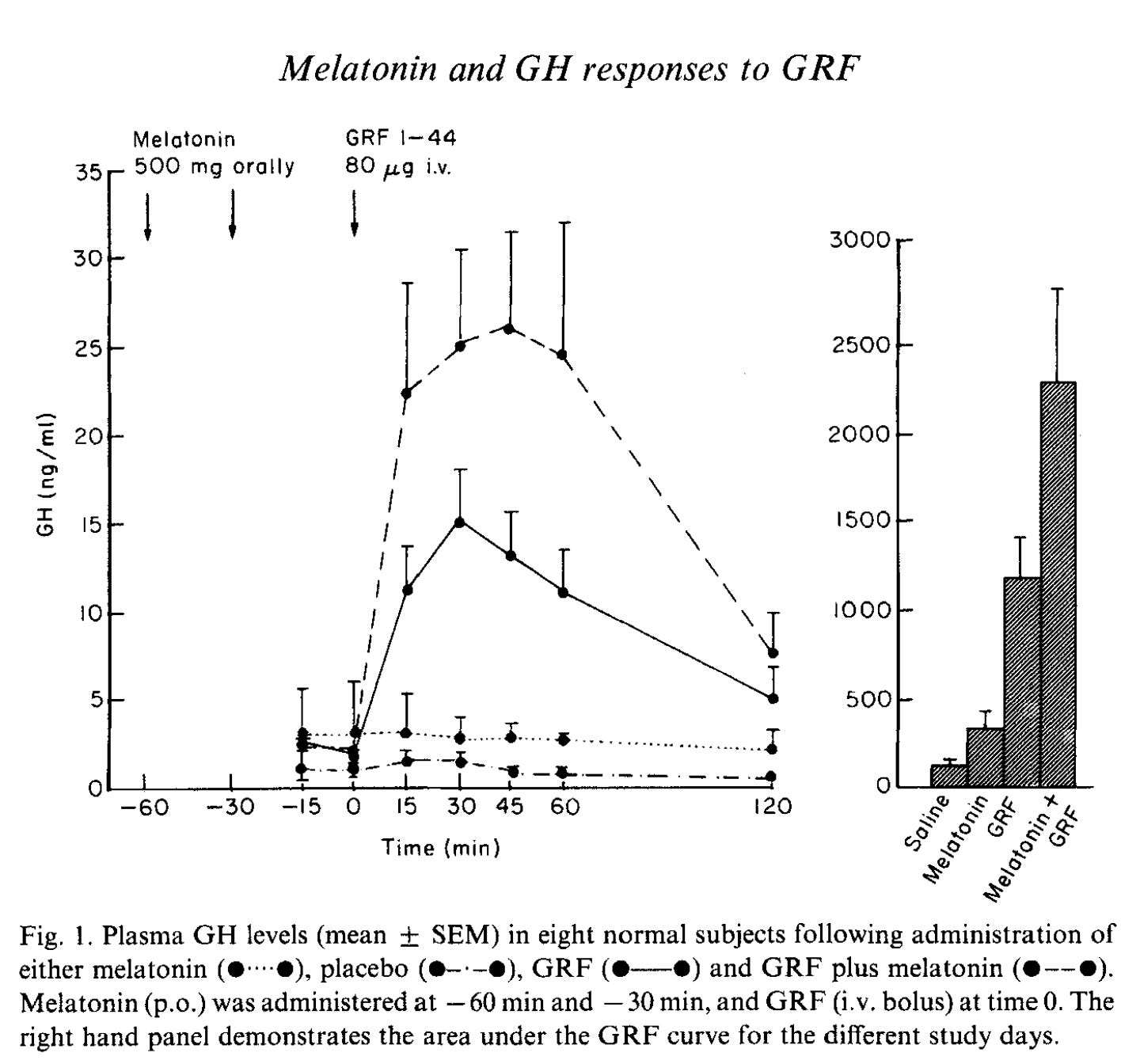
Valcavi and colleagues demonstrated this directly in 1987 by giving subjects oral melatonin before administering exogenous GHRH. Basal GH was higher with melatonin than without it, and the GH response to GHRH was significantly larger, particularly at submaximal GHRH doses. The potentiation was greatest precisely when the GHRH signal wasn’t already overwhelming the system, which is exactly the context you’re in when you’re running a secretagogue at a moderate dose rather than pushing the system to its limit.
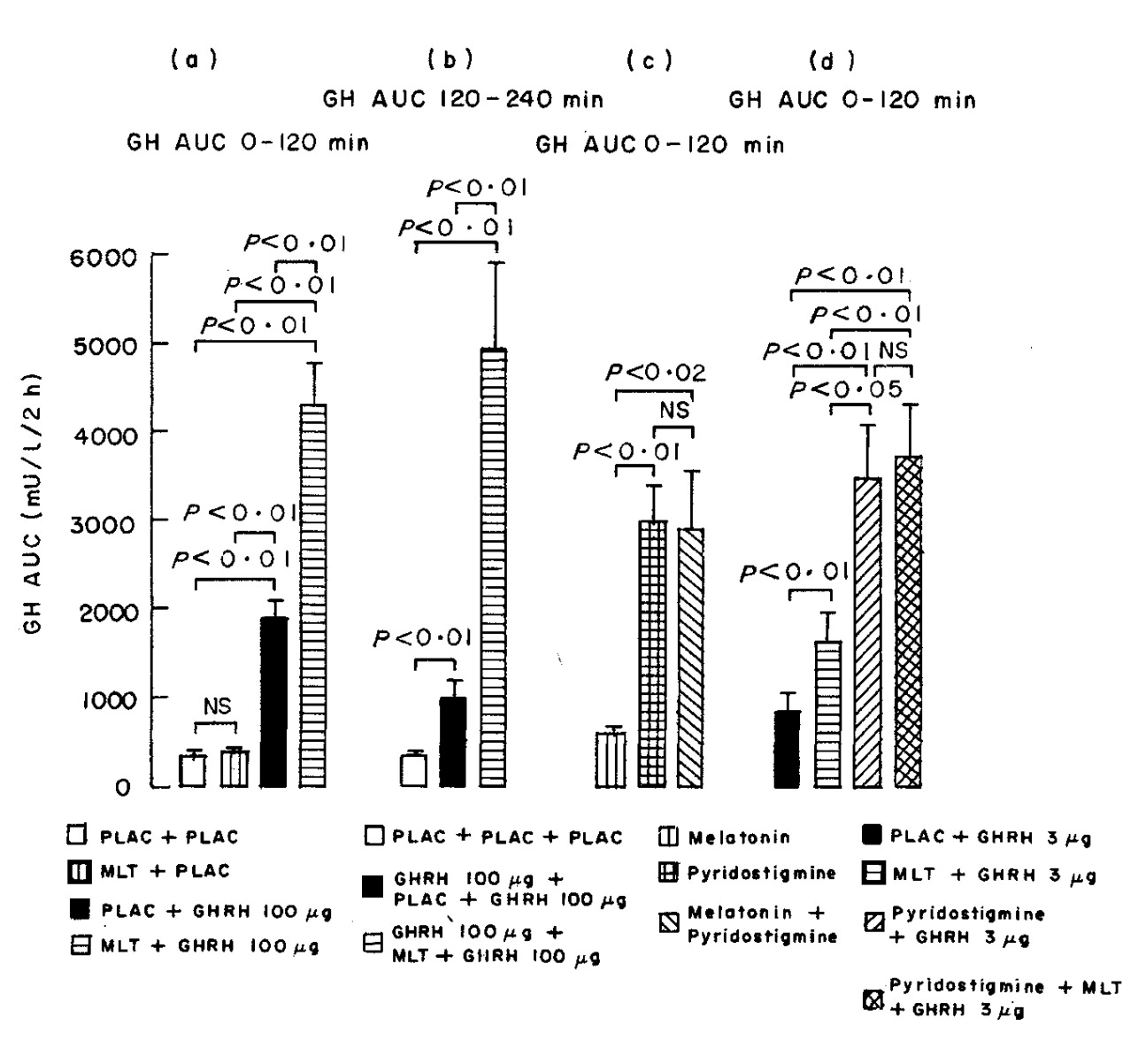
The mechanistic fingerprint comes from a study comparing melatonin directly to pyridostigmine, a drug with an established record as a somatostatin inhibitor. When researchers gave 10 mg of melatonin before a GHRH challenge, GH output roughly doubled compared to GHRH alone. Pyridostigmine produced almost the same potentiation pattern. When they combined both agents, GH did not increase further. They were working through the same pathway and had saturated it completely.
Pairing Melatonin with a Secretagogue: The Multi-Pathway Approach
Most protocols I build attack a single outcome through multiple independent mechanisms rather than pushing one agent to its limit. Lower individual doses, independent pathways, additive results without additive side effects. You see this with GLP-1 microdosing and it applies here just as directly.
Tesamorelin is typically studied and prescribed at 2 mg daily for HIV-associated lipodystrophy. For someone using it for body composition or recovery without that indication, 2 mg is a high starting point. The water retention that comes at higher doses is one of the main reasons people stop early. Utilizing tesamorelin at 1 mg gives you a clear GHRH signal at a dose where side effects stay manageable, and melatonin handles the somatostatin side by reducing the opposition that would otherwise blunt the pituitary’s response. The pituitary receives a GHRH signal with less resistance, and GH output reflects that.
The Valcavi data showed the greatest potentiation at submaximal GHRH doses, which is exactly the context this approach creates. When you’re not saturating the system with tesamorelin at maximum dose, melatonin’s somatostatin inhibition has room to produce a meaningful increase. Running both agents at moderate doses through separate pathways is where this combination earns its case.
Dosing, Timing, and Why I Cycle Tesamorelin
Melatonin dosing for GH purposes looks nothing like melatonin dosing for sleep. At 0.5 to 5 mg you get modest modulation of nocturnal GH patterns. At 10 mg the pyridostigmine comparison study shows roughly doubled GH response to GHRH. At 1 gram the Valcavi data shows the strongest potentiation on record in humans, and the dose-response relationship runs across several orders of magnitude.
For me, I prefer 100 mg nightly. The rationale for landing there is that 10 mg produces a meaningful effect in controlled settings, the gram-level data represents the upper bound of what has been tested, and 100 mg sits in a range where you’re well above the threshold for modest effects without taking on the full side effect profile of the highest experimental doses. There are no controlled trials at exactly 100 mg, so this is informed positioning on a dose-response curve rather than a number pulled directly from a protocol paper.
Taking melatonin at night alongside your secretagogue in a fasted state puts melatonin’s somatostatin inhibition to work precisely when your natural nocturnal GH pulsatility is already active.
The most common side effect is morning grogginess, which is dose-dependent and tends to resolve within one to two weeks as your body adapts. If it persists, dropping the dose is the first adjustment to make.
On cycling: I run tesamorelin 5 days on, 2 days off. The water retention from tesamorelin, which varies from person to person, accumulates with continuous use and can improve on the off days, though it doesn’t necessarily resolve completely. The main reason for the cycling, if I’m being honest, is injection fatigue. Receptor desensitization with chronic high-dose melatonin is sometimes cited as a reason to cycle, but the 2025 case report showing sustained GH and IGF-1 elevation throughout chronic melatonin use suggests the axis keeps responding without meaningful adaptation. Cycling high-dose receptor ligands is still sound pharmacology, and the practical reasons are sufficient on their own.
The Real-World Test
How much this stack moves your IGF-1 depends on a few variables. This combination is built around a GHRH analog. If you're running ipamorelin or a GHRP, you're hitting a different receptor and the literature supporting this specific interaction does not apply as directly.
The IGF-1 response to a given GH signal depends on your insulin sensitivity and liver function. A low-insulin environment from fasting or ketosis actually suppresses liver IGF-1 output, so someone eating a higher-carb diet with more insulin signaling available would likely see a larger IGF-1 response to the same protocol. Baseline somatostatin tone also varies between individuals, which means the size of the effect melatonin produces on GH pulsatility is not uniform. Sleep quality is another variable, since the majority of natural GH pulsatility happens during deep sleep and melatonin's amplification effect has less to work with if your sleep architecture is poor.
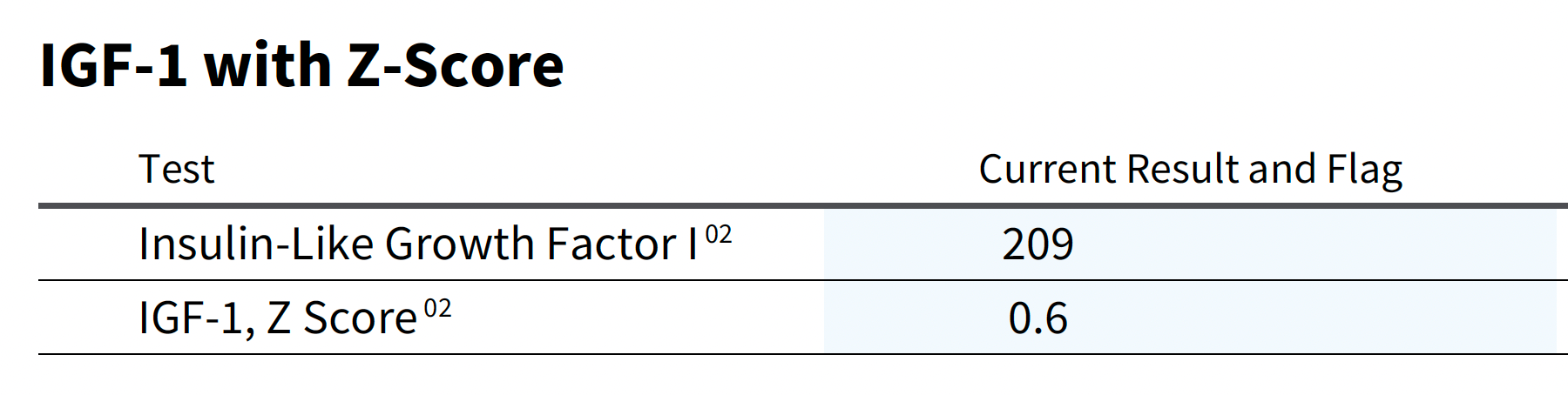
I ran this experiment on myself using Tesamorelin at 1 mg, 5 days on 2 days off, paired with 100 mg of melatonin nightly, in a deliberate low-insulin state through extended fasting and ketosis. My starting IGF-1 was 117, which sits near the low end of the reference range for a man my age, further dampened by the metabolic environment I was running.
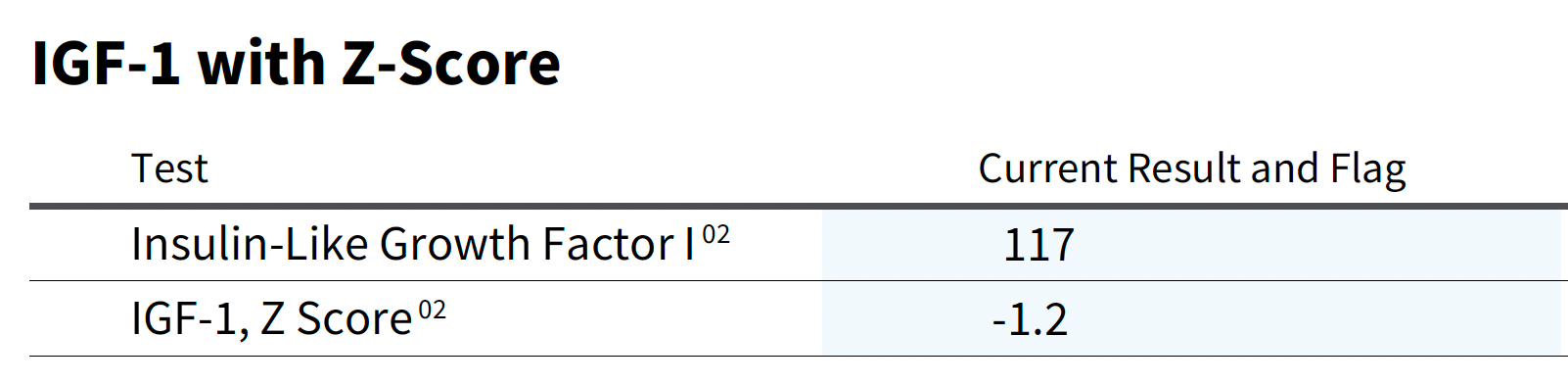
This baseline already had two things working against it. The fasting and ketosis were actively suppressing liver IGF-1 output through reduced insulin signaling, and 117 is low for a 32-year-old to begin with. After several weeks on the full stack, it came back at 209.
That's a nearly 100-point swing in an environment designed to keep IGF-1 down. Tesamorelin was driving the GHRH signal, melatonin was reducing the somatostatin opposition to that signal, and the pituitary was firing more completely with each pulse. The liver responded with more IGF-1 output, and that response was strong enough to overcome a metabolic environment that would otherwise suppress it.
Why This Stack Makes Sense
Most people running growth hormone secretagogues are thinking about one variable at a time. Dose the peptide higher, wait for better results, manage the side effects that follow. The somatostatin side of the equation gets almost no attention, and melatonin gets none at all. A molecule that costs a few dollars a month, has a standalone case as one of the better mitochondrial antioxidants we know of, and has human data going back over fifty years showing it directly amplifies GH output is sitting in the sleep aisle getting ignored by people who would genuinely benefit from it.
The stack works the way it does because each input addresses a different bottleneck in the same system. Tesamorelin provides the GHRH signal. Melatonin removes the somatostatin opposition to that signal. Deliberate insulin management creates the metabolic environment where the pituitary and liver can respond fully. Three independent inputs, each at a moderate dose, each working through a separate pathway, producing an outcome that pushing any single one of them harder would not have matched. Tesamorelin is not cheap, and running it at 1 mg instead of 2 mg cuts your peptide cost in half. Spending a few dollars a month on high-dose melatonin to make that lower dose perform better is one of the more straightforward value trades in this space.
If you’re already on a secretagogue, start at 10 mg nightly taken alongside your peptide in a fasted state. The dose-response data supports going higher if you’re tolerating it well and not waking up groggy. You’re getting mitochondrial antioxidant protection. You’re getting better sleep. You’re getting amplified GH output through a mechanism that runs you less than $10 a month. For a molecule that most people only think about when they can’t fall asleep, that’s a lot of return on a very small investment.
Link to Original Article - https://galizaidy.substack.com/p/supercharge-your-tesamorelin-with